PRP Therapy as an Alternative to Arthroscopic Knee Surgery
Explore how PRP injections can replace arthroscopic knee surgery for meniscus tears and knee OA. Research-backed guide on outcomes and candidacy.
April 2, 2026
Arthroscopic knee surgery is one of the most common orthopedic procedures in the United States, with over 700,000 performed each year. For decades it was the default treatment for meniscus tears, cartilage damage, and degenerative knee conditions. But a growing body of clinical evidence, including landmark randomized trials published in the New England Journal of Medicine, has shown that arthroscopic debridement and lavage often provide no more benefit than physical therapy alone for degenerative knee problems.1
That shift in the evidence has opened the door for biological treatments like platelet-rich plasma (PRP). If you have a meniscus tear, early osteoarthritis, or chronic knee pain and have been told arthroscopic surgery is the next step, PRP therapy may offer comparable or better results without the risks, recovery time, or cost of surgery.
This guide covers what the research says about PRP injections as an alternative to arthroscopic knee procedures, which patients benefit most, and when surgery is still the right call.
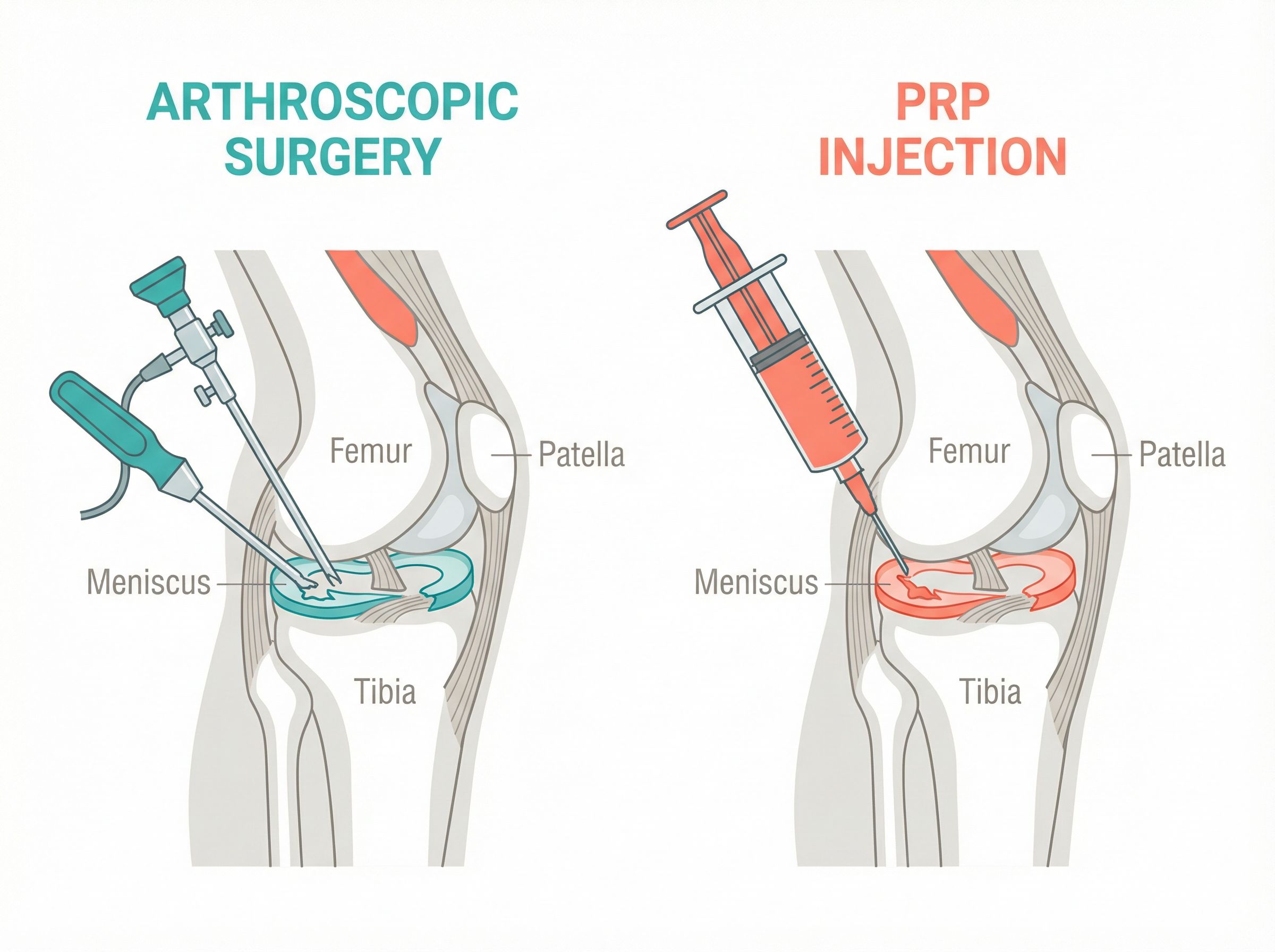
PRP therapy offers a non-surgical alternative to arthroscopic knee procedures for degenerative conditions.
The Problem with Arthroscopic Knee Surgery for Degenerative Conditions
Arthroscopic knee surgery encompasses several procedures, including partial meniscectomy (trimming torn meniscus tissue), debridement (cleaning up damaged cartilage and loose bodies), lavage (flushing the joint), and chondroplasty (smoothing roughened cartilage surfaces). These procedures are performed through small incisions using a camera and miniature surgical instruments.
For acute traumatic injuries in young, active patients, arthroscopic repair remains valuable. The issue lies with the far more common scenario: degenerative meniscus tears and osteoarthritis in middle-aged and older adults.
What the Landmark Trials Showed
The Moseley trial, published in the New England Journal of Medicine in 2002, randomized 180 patients with knee osteoarthritis to receive arthroscopic debridement, arthroscopic lavage, or sham surgery (skin incisions only, without inserting the arthroscope). At no point during the two-year follow-up did either surgical group report less pain or better function than the placebo group.1
The Kirkley trial, also published in the New England Journal of Medicine in 2008, confirmed these findings. Patients randomized to arthroscopic surgery plus optimized physical therapy showed no greater improvement in WOMAC scores at two years than those who received physical therapy alone.2
The Sihvonen trial in 2013 extended this evidence to degenerative meniscus tears specifically, finding that arthroscopic partial meniscectomy provided no benefit over sham surgery for patients with degenerative medial meniscus tears.
A Cochrane Collaboration review concluded there is "gold level evidence that arthroscopic debridement has no benefit" for knee osteoarthritis.2 Many insurers now classify routine debridement and lavage for osteoarthritis as not medically necessary.
Surgery Risks and Costs
While arthroscopic knee surgery is considered low risk, complications occur in up to 1% of cases, including infection, blood clots, nerve or blood vessel injury, and anesthesia-related events. A large study of 700,000 arthroscopic partial meniscectomies found a 0.317% rate of serious complications within 90 days, including pulmonary embolism, myocardial infarction, stroke, and infection requiring additional surgery.3
Recovery from arthroscopic meniscectomy takes 4 to 6 weeks for a return to normal activities. More complex repairs require 3 to 6 months. The average cost ranges from $5,000 to $15,000 depending on the facility, geographic area, and whether the procedure is performed in a hospital or ambulatory surgery center.4
Perhaps most concerning is the long-term consequence: partial meniscectomy accelerates the progression toward knee osteoarthritis by removing tissue that serves as a critical shock absorber. This creates a cycle where surgical treatment of a degenerative tear contributes to the very condition it was meant to address.
How PRP Works as a Non-Surgical Alternative
Platelet-rich plasma is a concentrated preparation drawn from your own blood. A small sample is processed in a centrifuge to isolate the platelet-rich layer, which is then injected directly into the knee joint or, in some protocols, directly into the meniscus tear under ultrasound or fluoroscopic guidance.
Platelets release growth factors including platelet-derived growth factor (PDGF), transforming growth factor beta (TGF-B), and vascular endothelial growth factor (VEGF). These growth factors reduce inflammation, stimulate tissue repair, improve synovial fluid quality, and may promote meniscal healing in areas with limited blood supply.
The inner two-thirds of the meniscus, known as the white-white zone, has almost no blood supply, which is why tears in this region heal poorly on their own. PRP delivers concentrated healing factors directly to these avascular areas, potentially enabling repair that the body cannot accomplish without intervention.
According to PubMed, a 2025 systematic review and meta-analysis by Dave et al. published in the Journal of Orthopaedics examined 8 comparative studies involving 354 patients who underwent meniscus repair with or without PRP augmentation. The results were striking: patients who received PRP augmentation had a significantly lower re-tear/failure rate of 18.2% compared to 30.5% in patients who underwent repair without PRP (P = 0.0188). There were no significant differences in wound complications or infection rates between the two groups. DOI5
This means PRP augmentation cut the meniscus repair failure rate by roughly 40%, a clinically meaningful difference that could spare patients from revision surgery.
PRP as Standalone Treatment for Degenerative Meniscus Tears
According to PubMed, a 2024 systematic review by Elphingstone et al. evaluated 10 studies with 686 patients receiving PRP for nonoperative management of degenerative meniscal tears. Most studies demonstrated improved pain and functionality by 3 months that persisted for at least one year. Within the intra-articular and intra-meniscal injection groups, 30% to 70% of patients were radiographically stable, and 40% to 60% demonstrated interval healing on follow-up imaging. Studies that tracked arthroscopy rates found lower failure rates and greater arthroscopy-free survival time in PRP-treated patients compared to controls. DOI6
The authors concluded that PRP appears to be a safe and efficacious treatment strategy for degenerative meniscal pathology, noting that both intra-articular and intra-meniscal injection approaches showed benefits.
PRP vs. Other Non-Surgical Treatments for Knee OA
According to PubMed, a comprehensive 2024 meta-analysis by Oeding et al. in The American Journal of Sports Medicine pooled data from randomized controlled trials involving 1,993 patients. PRP demonstrated significantly higher rates of successful outcomes compared to hyaluronic acid (OR 2.19, P = .002), higher rates of symptom relief versus all alternative non-operative treatments (OR 1.55, P = .019), lower rates of needing reintervention (OR 2.17, P = .002), and more frequent achievement of the minimal clinically important difference for pain improvement (OR 6.19, P = .007). The authors noted that these pooled treatment effects are "more robust than approximately half of all comparable meta-analyses in medicine and health care." DOI7
PRP After Arthroscopy for Early OA
According to PubMed, a 2025 cohort study by Giusti et al. compared umbilical cord-derived PRP to adipose tissue-derived mesenchymal stem cells in 225 patients following debridement and lavage arthroscopy for early-stage knee OA (Kellgren-Lawrence grade I-II). Both groups showed significant functional and pain improvements from baseline at all follow-up points. The PRP group demonstrated superior pain reduction at 3 and 6 months (P = .042 and P = .0065, respectively), with comparable functional scores at 12 months. DOI8
The Shift in Expert Opinion
According to PubMed, a 2025 editorial commentary in Arthroscopy by Suarez-Ahedo stated that based on emerging data from high-quality double-blinded randomized trials, "we may now recognize the superiority of PRP as an alternative to other biologic therapies" and called for PRP to be "placed at the top of the list" in the hierarchy of intra-articular treatments for knee osteoarthritis. DOI9
PRP vs. Corticosteroid Injections
Corticosteroid injections remain the most commonly prescribed injection for knee pain, but they offer only temporary relief (typically 4 to 8 weeks) and repeated use may accelerate cartilage loss. PRP works through a fundamentally different mechanism, delivering growth factors that support tissue repair rather than simply suppressing inflammation.
Multiple head-to-head trials have shown that while corticosteroids provide faster initial relief, PRP produces superior outcomes at 6 and 12 months. For a detailed comparison, read our guide on PRP vs. cortisone injections.
PRP delivers concentrated growth factors directly to the meniscus tear to promote healing.
Who Should Consider PRP Instead of Arthroscopic Surgery?
Based on the current evidence, PRP may be a strong alternative to arthroscopic surgery for patients in the following categories.
Degenerative meniscus tears in patients over 40. This is where the evidence against arthroscopy is strongest and the evidence for PRP is most compelling. If your meniscus tear is associated with degenerative changes rather than acute trauma, PRP offers comparable or better outcomes without removing protective meniscal tissue.6
Early to moderate knee osteoarthritis (Kellgren-Lawrence grade 1-3). Patients with some remaining cartilage respond best to PRP. The Oeding meta-analysis showed PRP outperformed all alternative non-operative treatments for knee OA, with lower rates of needing subsequent intervention.7
Failed conservative treatment. If physical therapy, oral anti-inflammatories, and activity modification have not provided adequate relief, PRP represents a logical next step before considering surgery.
Patients wanting to preserve meniscal tissue. Unlike partial meniscectomy, which removes damaged tissue and accelerates osteoarthritis progression, PRP aims to promote healing while preserving the meniscus intact.
Patients who are not good surgical candidates. Those with medical comorbidities that increase surgical risk, or those who cannot afford the recovery time from surgery, may benefit from PRP as a lower-risk alternative.
For patients with meniscus tears or ACL injuries, PRP can also serve as an adjunct to rehabilitation or as a bridge treatment.
What Does PRP Treatment Look Like?
A typical PRP protocol for knee conditions involves 1 to 3 injections spaced 2 to 4 weeks apart. The procedure is performed in an office setting and takes approximately 30 to 45 minutes, including blood draw, centrifuge processing, and ultrasound-guided injection.
For meniscus tears specifically, some providers use intra-meniscal injection (directly into the tear) in addition to or instead of standard intra-articular injection. The Elphingstone systematic review found that both approaches showed benefits, with intra-meniscal injection showing particularly promising rates of radiographic healing.6
Most patients experience mild soreness at the injection site for 1 to 3 days. There is no hospitalization, no anesthesia, and no restriction from weight-bearing. Most people return to normal activities within a few days.
Cost Comparison: PRP vs. Arthroscopic Knee Surgery
A single PRP treatment session typically costs between $500 and $2,500. A full treatment course of 1 to 3 sessions runs approximately $500 to $7,500 total.
Arthroscopic knee surgery costs between $5,000 and $15,000, not including physical therapy, follow-up visits, and lost work time during the 4-to-6-week recovery period.4 For meniscus repair (as opposed to meniscectomy), costs can run higher, and the recovery period extends to 3 to 6 months.
Even accounting for the possibility that PRP treatment may need to be repeated, the total cost over several years typically remains well below a single arthroscopic procedure. For a comprehensive breakdown of PRP pricing, visit our PRP cost guide.
When Arthroscopic Surgery Is Still the Right Choice
PRP is not appropriate for every knee condition. Arthroscopic surgery remains the preferred treatment in several specific situations.
Acute traumatic meniscus tears in young athletes. Bucket-handle tears, displaced tears causing mechanical locking, and tears in active patients under 40 with an otherwise healthy knee often warrant surgical repair to restore full knee function.
Loose bodies causing locking or catching. When free-floating fragments of cartilage or bone are physically blocking knee movement, arthroscopic removal provides immediate mechanical relief that PRP cannot address.
ACL reconstruction. Patients undergoing ACL reconstruction who have concurrent meniscus tears typically benefit from surgical repair at the same time. PRP may be used as an augmentation to improve healing rates in these cases.5
Failed non-operative treatment including PRP. If PRP and other conservative measures have not provided adequate relief after a reasonable trial period (typically 3 to 6 months), arthroscopic evaluation and treatment may be the appropriate next step.
The decision should always be made collaboratively between you and your orthopedic specialist, based on imaging findings, symptom severity, activity level, and your personal goals.
The Bottom Line
The evidence supporting PRP as an alternative to arthroscopic knee surgery has strengthened considerably. For degenerative meniscus tears and knee osteoarthritis, landmark trials have shown that arthroscopy often provides no more benefit than physical therapy alone, while PRP has demonstrated meaningful improvements in pain, function, and meniscal healing across multiple systematic reviews and randomized trials. PRP cuts meniscus repair failure rates by 40%, outperforms hyaluronic acid and other injectables in meta-analyses, and achieves these results without surgery, without downtime, and at a fraction of the cost.
For the right patient, PRP is not just a reasonable alternative to arthroscopic knee surgery. Leading researchers now argue it should be the first-line injectable treatment for knee osteoarthritis.
1. Moseley JB, O'Malley K, Petersen NJ, et al. A controlled trial of arthroscopic surgery for osteoarthritis of the knee. N Engl J Med. 2002;347(2):81-88.
2. Kirkley A, Birmingham TB, Litchfield RB, et al. A randomized trial of arthroscopic surgery for osteoarthritis of the knee. N Engl J Med. 2008;359(11):1097-1107.
3. Abrams GD, Frank RM, Gupta AK, et al. Adverse outcomes after arthroscopic partial meniscectomy: a study of 700,000 procedures in the national Hospital Episode Statistics database for England. Arthroscopy. 2018;34(12):3265-3272.
4. Knee arthroscopy cost data. NewChoiceHealth.com. Accessed April 2026.
5. Dave U, Rubin J, Chang N, et al. Platelet rich plasma augmentation for meniscus repair reduces failure but not complication rates or outcomes: a systematic review and meta-analysis. J Orthop. 2025;73:62-71. DOI
6. Elphingstone JW, Alston ET, Colorado BS. Platelet-rich plasma for nonoperative management of degenerative meniscal tears: a systematic review. J Orthop. 2024;54:67-75. DOI
7. Oeding JF, Varady NH, Fearington FW, et al. Platelet-rich plasma versus alternative injections for osteoarthritis of the knee: a systematic review and statistical fragility index-based meta-analysis of randomized controlled trials. Am J Sports Med. 2024;52(12):3147-3160. DOI
8. Giusti S, Cerulli S, Giacinto E, Adriani E. Is umbilical cord-derived platelet-rich plasma a valid alternative to conventional orthobiologics post-knee arthroscopy? Adv Orthop. 2025;2025:8026214. DOI
9. Suarez-Ahedo C. Editorial commentary: Should platelet-rich plasma be the new standard? Reframing biologic strategies for knee osteoarthritis. Arthroscopy. 2025;41(12):5319-5320. DOI
10. Super JT, Murray IR, Tollefson LV, et al. Biologic augmentation strategies in meniscus repair: a Delphi study. Knee Surg Sports Traumatol Arthrosc. 2026. DOI
Find a PRP Specialist Near You
Search our verified directory of orthopedic PRP providers who specialize in regenerative treatments.