Explore how PRP injections can treat achilles tendinitis. Learn about platelet-rich plasma therapy benefits, recovery, and results for achilles tendinitis.
Achilles tendinitis, pain, stiffness, and swelling along the back of the ankle, is one of the most common and frustrating overuse injuries. Unlike many other tendon conditions where cortisone injections are a first line of defense, cortisone is widely avoided near the Achilles due to the risk of tendon damage. PRP (Platelet-Rich Plasma) has emerged as an alternative that works with the body's own healing biology rather than suppressing it. Here is what the evidence shows.
What Is Achilles Tendinitis?
The Achilles tendon is the largest and strongest tendon in the body, connecting the calf muscles to the heel bone. Achilles tendinitis, more precisely called Achilles tendinopathy, refers to degeneration and pain in this tendon, typically from repetitive loading during running, jumping, or prolonged standing.
The most common form affects the midportion of the tendon, about 2–6 cm above the heel. A second type, insertional tendinopathy, occurs where the tendon attaches to the heel bone. Like other tendinopathies, the underlying problem is degenerative, the tendon tissue breaks down faster than it repairs, leading to chronic pain and structural weakness.
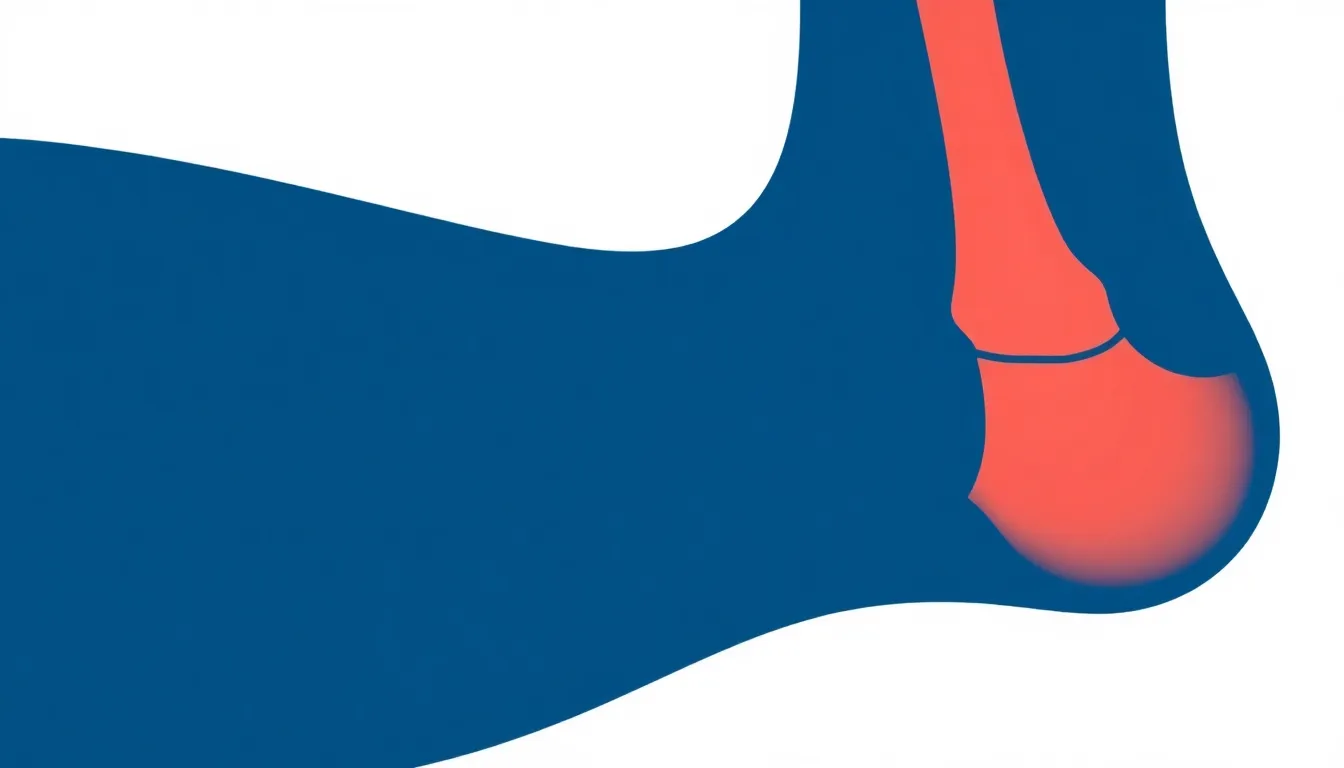
Achilles tendon anatomy showing the midportion, the most common site of tendinopathy, and its connection between the calf muscles and heel bone.
Common Symptoms
The hallmark of Achilles tendinopathy is pain and stiffness along the back of the leg near the heel. Morning stiffness is classic, the tendon feels tight and painful for the first several minutes of walking after rest. Pain is aggravated by running, climbing stairs, or prolonged standing, and may ease with gentle activity but return after exercise. Tendon thickening or a tender nodule may be palpable in chronic cases.
Why Cortisone Is Avoided Near the Achilles
Cortisone (corticosteroid) injections are a common tool for many musculoskeletal conditions, but they carry significant risk near the Achilles tendon. Intratendinous steroid injection causes collagen necrosis and reduces tendon strength, a serious concern given the Achilles already bears up to eight times body weight during running. For this reason, most orthopedic specialists avoid corticosteroid injection at the Achilles, particularly for midportion tendinopathy.
PRP presents a fundamentally different risk profile. Because it is derived from the patient's own blood, it carries no risk of tendon weakening, and its growth factor content actively promotes new collagen synthesis and tissue repair.
Treatment
Mechanism
Time to Effect
Best For
Key Limitation
PRP Injection
Growth factors stimulate tendon repair
6–12 weeks
Chronic cases resistant to PT
Mixed RCT evidence; no guaranteed response
Eccentric Exercise
Loads and remodels the Achilles progressively
8–12 weeks
First-line for all patients
Slow; requires adherence
Cortisone Injection
Suppresses inflammation short-term
1–2 weeks
Generally AVOIDED near Achilles
Tendon weakening and rupture risk
Shockwave Therapy (ESWT)
Stimulates repair via acoustic energy
6–12 weeks
Midportion tendinopathy
Multiple sessions; variable results
Surgical Debridement
Removes degenerative tissue directly
3–6 months recovery
Failed all non-surgical options
Invasive; long recovery
How PRP Therapy Works for Achilles Tendinopathy
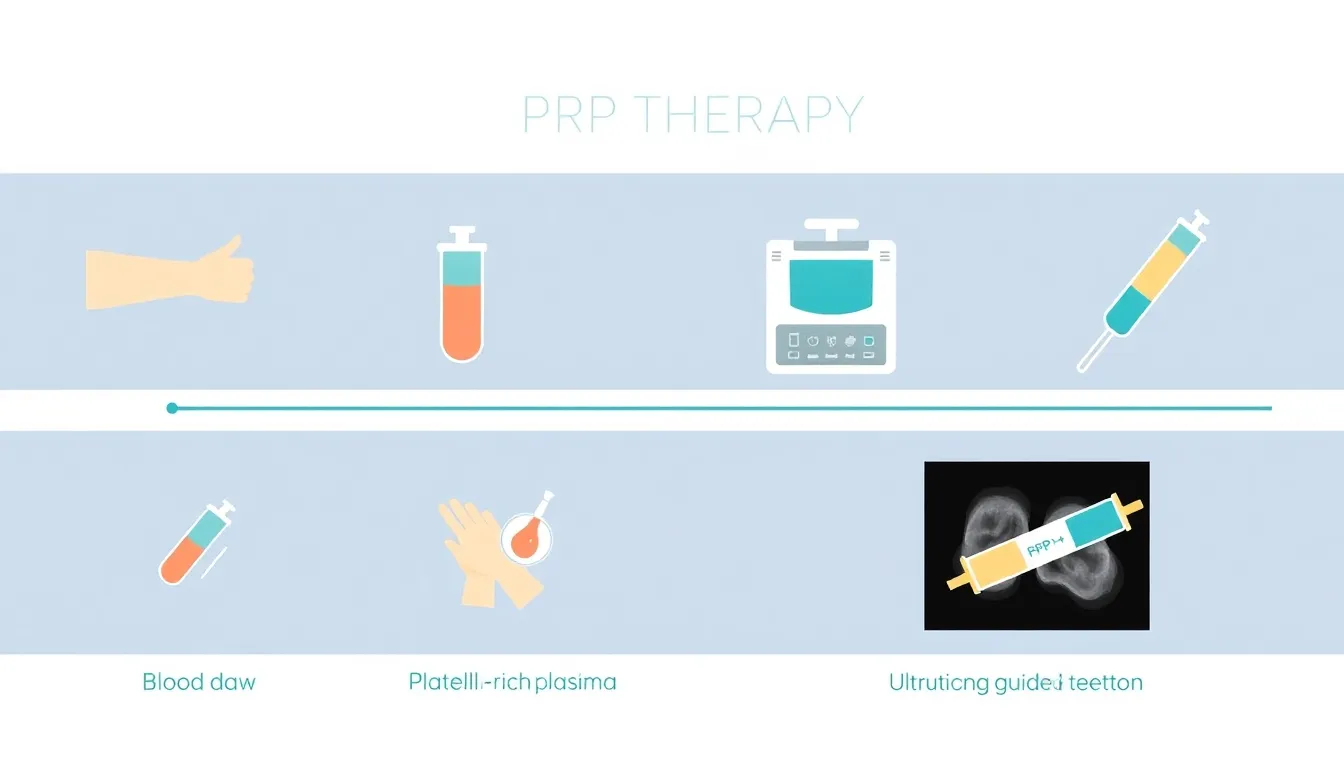
PRP is prepared by drawing a small blood sample, concentrating the platelet-rich portion through centrifugation, and injecting it into the degenerative zone of the tendon under ultrasound guidance. The concentrated growth factors, PDGF, TGF-β, VEGF, and others, stimulate the body's repair mechanisms to produce new collagen and restore tendon structure.
Ultrasound imaging is used both to identify the area of maximal degeneration and to guide the needle precisely into the target tissue. PRP is most commonly used for chronic midportion Achilles tendinopathy, cases that have not responded to eccentric exercise, physical therapy, or other conservative measures.
The four-step PRP preparation process: blood draw, centrifugation, platelet concentration, and ultrasound-guided injection into the Achilles tendon.
A broader 2025 systematic review and meta-analysis of 13 studies including 697 patients2 found more positive results: a significant reduction in pain (VAS scores) and a return-to-activity rate of 85% (95% CI: 65–98%) following PRP treatment. Patient satisfaction reached 72%. The authors noted that high variability in PRP preparation methods contributed to heterogeneous outcomes across studies.
The honest picture: evidence for PRP in Achilles tendinopathy is more mixed than for some other tendinopathies (such as knee osteoarthritis or lateral epicondylitis). High-quality placebo-controlled trials have not consistently demonstrated superiority over sham injection. However, real-world series consistently report meaningful improvement and high patient satisfaction, and crucially, PRP provides a viable treatment path for the majority of patients for whom cortisone is not a safe option.
Who Is a Good Candidate?
PRP is most appropriate for patients with chronic midportion Achilles tendinopathy, typically those with symptoms lasting more than 3 months that have not adequately responded to eccentric exercise (the primary non-surgical treatment), physical therapy, load management, or orthotics. Patients who need a non-surgical injection option and cannot use cortisone safely are also strong candidates.
Diagnostic ultrasound is typically used before treatment to confirm the location and extent of tendon degeneration, identify any structural tear, and guide injection placement.
What to Expect After PRP for Achilles Tendinopathy
An increase in Achilles pain and stiffness for 3–7 days following the injection is common and expected, this is part of the inflammatory healing response triggered by PRP. High-impact loading (running, jumping) should be avoided for 2 weeks. Physical therapy and a progressive eccentric loading program are recommended starting at 2–4 weeks to guide tendon remodeling.
Improvement typically begins at 6–8 weeks, with continued progress through 3–6 months. Most clinical series report a single injection, with a second injection considered at 6–8 weeks if the initial response is incomplete.
1. Ling SK, Mak CT, Lo JP, Yung PS. Effect of Platelet-Rich Plasma Injection on the Treatment of Achilles Tendinopathy: A Systematic Review and Meta-analysis. Orthop J Sports Med. 2024;12(11):23259671241296508. doi:10.1177/23259671241296508. PMID: 39611122.
2. Ahmed AE, et al. Efficacy of Platelet-Rich Plasma in Treatment of Achilles Tendinopathy: Systematic Review and Meta-Analysis. Cureus. 2025;17(2):e79692. doi:10.7759/cureus.79692. PMID: 40161095.
This content is for educational purposes only and does not constitute medical advice. Consult a qualified healthcare provider before starting any treatment.
Frequently Asked Questions
Find an Achilles Tendinopathy PRP Specialist
Search our verified directory of orthopedic PRP providers who treat Achilles tendon pain and chronic tendinopathy.