Explore how PRP injections can treat disc degeneration. Learn about platelet-rich plasma therapy benefits, recovery, and results for disc degeneration.
Intervertebral disc degeneration is the structural breakdown of the cushioning discs between spinal vertebrae, and one of the most common sources of chronic axial low back pain. As discs lose water content and height over time, the diminished shock-absorbing capacity and resulting chemical irritation can generate persistent pain that outlasts most conventional treatments. Platelet-rich plasma (PRP) therapy offers an intradiscal injection approach aimed at slowing disc degeneration and reducing discogenic pain by delivering regenerative growth factors directly to the nucleus pulposus.
What Is Disc Degeneration?
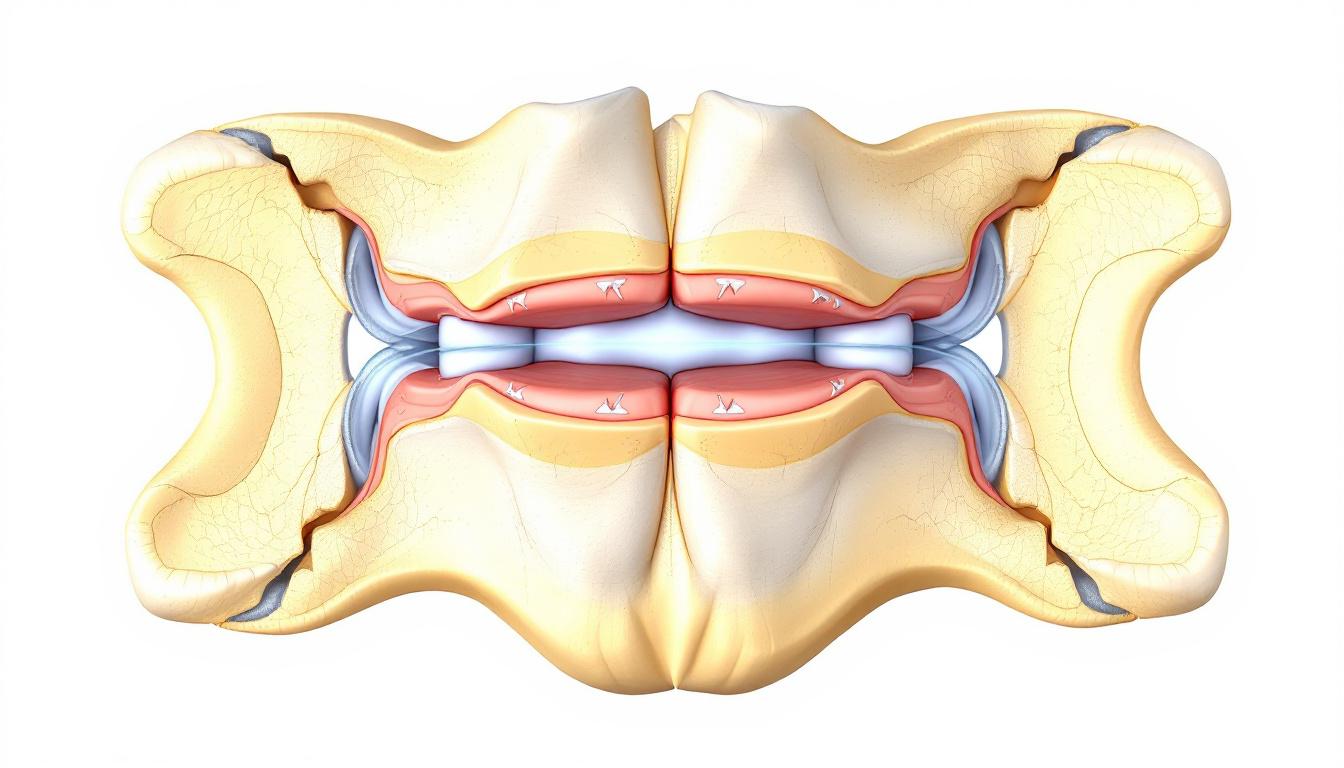
Each intervertebral disc consists of a gel-like nucleus pulposus surrounded by the fibrous annulus fibrosus. In youth, the nucleus is roughly 80% water, giving it the capacity to distribute compressive forces evenly. With age and accumulated mechanical stress, disc cells progressively lose their ability to synthesize proteoglycans (the molecules that retain water), causing the nucleus to dehydrate, flatten, and fissure.
As disc height decreases, facet joint load increases and foraminal space narrows, potentially compressing exiting nerve roots. Damaged discs also release inflammatory mediators including IL-1β, TNF-α, and substance P that sensitize nearby nociceptors, creating a dual pain generator: structural (mechanical instability) and chemical (inflammatory discharge).
Degenerative disc disease (DDD) is not a disease but a normal aging process that becomes clinically significant when it causes persistent pain. Symptoms include deep, aching low back pain that worsens with prolonged sitting or bending and may radiate into the buttocks or thighs. MRI confirms the diagnosis through T2-weighted signal loss and reduced disc height.
Application
Injection Target
Evidence Level
Typical Protocol
Best Candidates
Disc Degeneration (DDD)
Nucleus pulposus (intradiscal)
Moderate, RCT (Tuakli-Wosornu 2016)
1–2 injections under fluoroscopy
Pfirrmann Grade III–IV; discogenic pain 6+ months; failed conservative care
How PRP Is Used for Disc Degeneration
Intradiscal PRP targets the nucleus pulposus directly, delivering a concentrated preparation of autologous platelets and growth factors, including PDGF, TGF-β, IGF-1, and VEGF, to the degenerating disc environment. This approach aims to:
Stimulate nucleus pulposus cell (NPC) proliferation and proteoglycan synthesis, potentially slowing the biochemical degeneration cascade
Reduce the intradiscal inflammatory cytokine load that sensitizes nociceptors and perpetuates discogenic pain
Promote annular repair at sites of fissuring
The procedure is performed under biplanar fluoroscopic guidance with the patient prone. After confirming disc level with imaging, the physician advances a needle into the nucleus pulposus using an oblique posterolateral approach, confirms placement with contrast, and slowly injects the PRP. The outpatient procedure takes 30–60 minutes including blood draw and centrifugation.
What the Research Shows
The landmark clinical study for intradiscal PRP was a prospective, double-blind, randomized controlled trial by Tuakli-Wosornu and colleagues (PM&R, 2016, PMID: 26835989). Patients with chronic discogenic low back pain confirmed by provocative discography were randomly assigned to intradiscal PRP or a contrast agent control. The PRP group demonstrated statistically significant improvements in functional disability and pain intensity at one month, with sustained gains through eight months of follow-up, results the control group did not replicate.
Levi et al. (2016) published an open-label pilot study of intradiscal PRP in seven patients with MRI-confirmed disc degeneration, reporting improvement in pain and disability scores at six months and supporting safety and tolerability of the procedure. Basic science studies have also shown that PRP enhances NPC viability and proteoglycan production in in vitro and animal disc models.
The evidence base remains smaller than for peripheral joint PRP applications, and intradiscal PRP is not yet a first-line standard of care. Patients should have a frank discussion with their physician about realistic expectations, procedure-specific risks, and the current state of evidence.
PRP vs. Epidural Injections
Epidural steroid injections (ESIs) deliver corticosteroid into the epidural space, reducing perineural inflammation most effectively in radiculopathy. They perform less consistently for purely discogenic pain, the medication reaches the outside of the thecal sac rather than the disc itself, and the anti-inflammatory effect is temporary.
Intradiscal PRP targets the disc directly and is designed to modify the pathological process rather than suppress symptoms. Where ESIs provide anti-inflammatory pain relief lasting weeks to months, PRP seeks to reduce the biochemical drivers of discogenic pain through tissue remodeling, an effect that may prove more durable.
Neither treatment replaces surgical intervention for structural spinal instability, severe foraminal stenosis, or significant neurological deficit. PRP is most appropriate for patients with isolated discogenic pain from moderate disc degeneration who have not responded to conservative care but are not yet surgical candidates.
Who Is a Good Candidate?
PRP is most appropriate for disc degeneration when:
Chronic axial low back pain has persisted for 6 or more months
MRI confirms moderate disc degeneration (Pfirrmann Grade III–IV) at one or two levels
Provocative discography or diagnostic blocks have confirmed the disc as the primary pain source
Physical therapy, activity modification, and oral medications have provided insufficient relief
No recent spinal surgery at the involved level, active infection, coagulopathy, or significant neurological compromise is present
Severe disc degeneration with near-complete height loss (Pfirrmann Grade V) may have insufficient viable disc tissue to respond to PRP. Smokers face reduced disc cell viability and may respond less robustly. The procedure is not appropriate for isolated radiculopathy or when the primary pain source is the facet joints rather than the disc.
What to Expect
Intradiscal PRP is performed as an outpatient procedure under fluoroscopic guidance, typically with light sedation or local anesthetic. After blood draw and centrifugation (approximately 15 minutes), the physician confirms needle placement in the nucleus pulposus using contrast visualization, then injects the PRP slowly.
Expect moderate back soreness for 3–7 days post-injection, an expected inflammatory healing response. Heavy lifting, bending, and twisting should be avoided for 2–4 weeks. Anti-inflammatory medications (NSAIDs, corticosteroids) should be held for at least 2 weeks to avoid blunting the platelet-mediated healing response.
Functional improvement typically begins at 6–8 weeks, with peak response at 3–6 months. A second injection may be considered at 8–12 weeks for partial responders. Physical therapy targeting core stabilization should begin at 2–4 weeks post-injection and is an integral part of the treatment program.
Sources
1. Tuakli-Wosornu YA, Terry A, Boachie-Adjei K, et al. Lumbar intradiscal platelet-rich plasma (PRP) injections: a prospective, double-blind, randomized controlled study. PM R. 2016;8(1):1-10. PMID: 26835989.
2. Levi D, Horn S, Tyszko S, Levin J, Hecht-Leavitt C, Walko E. Intradiscal platelet-rich plasma injection for chronic discogenic low back pain: preliminary results from a prospective trial. Pain Med. 2016;17(6):1010-1022. PMID: 26555810.
3. Navani A, Manchikanti L, Albers SL, et al. Responsible, safe, and effective use of biologics in the management of low back pain: ASIPP guidelines. Pain Physician. 2019;22(suppl1):S1-S74.
Frequently Asked Questions
Find a Disc Degeneration PRP Specialist Near You
Browse our directory of verified providers who offer intradiscal PRP injections for degenerative disc disease and chronic low back pain.